
 In this article featured in The Journal of Aesthetic Nursing, Dr Samantha Hills explains the benefits of treating various types of scars with different lasers, as well as the additional modalities for scar treatment.
In this article featured in The Journal of Aesthetic Nursing, Dr Samantha Hills explains the benefits of treating various types of scars with different lasers, as well as the additional modalities for scar treatment.
The formation of scar tissue is a natural bodily response to a dermal injury. With most deep wounds there will be some degree of scar formation and a variety of different scars can develop following surgery, trauma, and cutaneous inflammatory processes.
Scars are not harmful and do not require removal for medical reasons. However, they can be painful, itchy, limiting, and have a significant effect on a person psychologically, prompting patients to seek treatment. With the laser and light-based technologies available today, increasing evidence demonstrates the efficacy of these treatments in improving different varieties of scars, including keloids, hypertrophic scars, atrophic scars, and acne scars.2
Laser Scar Therapy
Laser scar therapy utilises photothermal energy to target intra- and extra-cellular structures within the scar tissue in order to improve the colour, and also stimulate the process of neocollagenesis and dermal remodelling. Rarely can a scar be removed completely using these methods, instead the aim is to reduce the appearance of scars and any discomfort caused mentally, physically and cosmetically.
Types of Lasers for Scar Treatment
Various types of lasers have been utilised in the treatment of scars for a number of years, including CO2, Nd:YAG, Pulse Dye and Er:YAG lasers.7 Lasers are chosen based on the severity of the scar, patient skin type and work according to the theory of selective photothermolysis. Most recently, fractional photothermolysis with ablative and non-ablative fractionated lasers have found use as effective treatments for scars2.
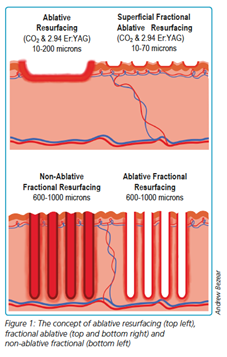
The Difference Between Ablative and Non-Ablative Lasers
The differences between ablative and non-ablative lasers as well as fractional and non-fractional delivery are based on the fundamental process of the target chromophore, photo-thermolysis and how the energy is delivered to the target area.
Ablative lasers are highly absorbed by water and cause the removal of material from the surface of the skin by vaporisation. In comparison, non-ablative lasers do not reach temperatures in the tissue to induce vaporisation, and as such, do not remove material. Instead, they deliver a controlled zone of thermal damage through epidermal and dermal heating.
Fractional Laser
Both non-ablative and ablative lasers can be administered via a fractional delivery system, meaning that the laser beam is divided into an array of microscopic laser beams much smaller in size than the original full beam. This fractional delivery can be produced in a number of ways, most commonly via a micro-lens array or a fractional scanner.
What Causes Scarring?
Excessive pulling or tension across a healing wound is a factor which may increase inflammation and scar formation, and if healing is delayed, for example, due to infection, this will increase the risk of a build-up of connective fibrous tissue, resulting in an increased likelihood of scarring.
The main distinction between scar tissue and normal skin is the amount of collagen it contains and the manner in which the collagen fibres are produced. The elongated collagen fibres are well arranged in normal skin. The structure of collagen fibres in scars, on the other hand, is disorganised and markedly different from the normal surrounding tissue. The collagen fibres become more tightly packed and more resistant to elimination by the natural enzymes released by the body as the scar ages.
The degree of scarring, including the size and depth of the wound, the blood supply to the region, the thickness and colour of the skin, and the direction of the scar, can be influenced by several variables. The age of individuals also significantly influences the development of scars. Younger skin, for example, appears to over-heal, resulting in bigger, darker scars compared to older skin. In addition, the location of the body where the wound takes place can impact the appearance of the scar, with the sternum being particularly prone to scar formation.

Types of Scars
There are numerous types of scars encountered when treating patients, the most common being atrophic, keloid, hypertrophic scars. Acne scars are also common and can present in a number of different ways.
Atrophic Scars
Atrophic scars can occur anywhere on the body and generally present as an indented scar that heals below the normal layer of skin tissue. The scar may be irregular, with jagged edges and a pitted, sunken appearance. Atrophic scars form when the skin is unable to regenerate tissue. Atrophic scars often appear after severe acne, chickenpox, surgery or accidents that cause underlying trauma to the area.
Keloid Scars
Keloid scars are abnormal scars that grow beyond the boundaries of the original injury, resulting from excess collagen at the injury site. They are generally pink to purple in colour, or may display hyperpigmentation. In some cases, extra scar tissue grows, forming smooth, hard growths. Often keloid scars can be much larger than the original wound. The most common areas where keloids form is the anterior chest, shoulders, ear lobes, cheeks, and skin overlying joints. Patients will often feel itching, hyperesthesia and pain. Despite the broad range of modalities available to treat scars, the treatment of keloid scars remains a challenging clinical dilemma for both patients and providers. Studies have shown that keloid formation can be prevented if anticipated with immediate silicone elastomer sheeting, taping to reduce skin tension or corticosteroid injections. Cryotherapy may be useful but should be reserved for smaller lesions.
Surgical removal of keloids can pose a high risk of recurrence unless combined with one or several modalities such as silicone elastomer sheeting, a non-invasive but time-intensive, first-line option for the treatment of keloids and hypertrophic scars.
Hypertrophic Scars
Hypertrophic scars are widened scars, usually raised and dark in colour, although unlike a keloid scar, they remain within the boundaries of the wound. They can continue to thicken for up to six months[13]. Unlike keloids, hypertrophic scars are smaller, and the colouring can fade over time. Hypertrophic scarring occurs after thermal and/or traumatic injury concerning the reticular dermis. The risk of hypertrophic scars forming, like keloid scars, can be reduced post-surgery, by use of silicone elastomer sheeting, pressure dressings or garments. This can be especially in the case of burns.
Acne Scars
Acne scars fall into an additional category. There are three main types of acne scars; ice pick scars, rolling scars and boxcar scars. Ice pick scars are very small, deep holes in the surface of your skin that look like the skin has been punctured with a sharp object, leaving behind what looks like little holes on the face. Rolling scars are caused by bands of scar tissue that form under the skin, giving the surface of the skin a rolling and uneven appearance – visibly you can see the skin dip. Boxcar scars are round or oval depressions or craters in the skin with parallel sidewalls. Despite the psychological stress acne scarring can place on an individual, treatment is generally regarded as cosmetic surgery and is not usually available on the NHS, therefore the demand is high for effective treatment within private clinics.
Other specific types of scars include post-operative scars, post-trauma scars, burn scars, post-infective scars or diabetic wound scars. In some instances, it’s possible to encounter combination scars such as hypertrophied post-op scars or keloid trauma wounds.
Treating Scars
 For the application of lasers for scar treatments, the theory of selective photo-thermolysis describes the means by which the skin’s chromophores (water, melanin, haemoglobin), are targeted by the use of an appropriate wavelength and pulse duration of a laser or light source. Generally, this is done to produce thermal damage to the target area, without damage to the surrounding tissues and structures.
For the application of lasers for scar treatments, the theory of selective photo-thermolysis describes the means by which the skin’s chromophores (water, melanin, haemoglobin), are targeted by the use of an appropriate wavelength and pulse duration of a laser or light source. Generally, this is done to produce thermal damage to the target area, without damage to the surrounding tissues and structures.
With the treatment of scars, ablative erbium-doped yttrium aluminium garnet (Er:YAG) (1540 nm) and Carbon Dioxide (CO2) (10,600 nm) lasers are commonly selected, with water being the target chromophore. CO2 and Er:YAG lasers are particularly effective in the treatment of scars due to their ability to smooth scar texture and stimulate collagen production,13 although patients and practitioners must consider the potential for significant downtime as re-epithelialization typically takes 4 to 7 days with Er: YAG and 7 to 10 days with the CO2 laser. While inducing more downtime than non-ablative lasers, they usually produce a higher degree of clinical improvement.
In particular, for the treatment of acne scars, previous head-to-head studies have suggested that CO2 laser produces superior results while Er: YAG is better tolerated with less downtime. Raised scars and shallow boxcar scars improve the most with laser resurfacing, whilst ice pick scars are more challenging to treat and may necessitate secondary resurfacing.
More recently, fractional ablative laser resurfacing has emerged as a popular treatment modality for scar therapy. In fractional ablative resurfacing, columns of energy create heat in the dermis, which works on the principle of injury and repair leading to reversible necrosis resulting in collagenases, angiogenesis and structural changes within the dermis and scar tissue. The microscopic thermal treatment zones are separated by surrounding untreated skin, resulting in rapid re-epithelialization and reduced downtime as only a fraction of skin is altered.[20] A double-blinded split-scar study by Tidwell et al. reported a significantly superior outcome with fractionated Er: YAG compared to fully ablative Er: YAG for surgical scar revision, with 94% of patients preferring the side of the scar treated with fractional ablative resurfacing.21 Another study showed fractional CO2 laser to be effective in treating atrophic traumatic scars in 70% of patients treated with six monthly sessions of fractional CO2 laser treatment.
Non-ablative fractional lasers have also been shown to significantly improve the pigmentation and thickness of surgical scars, atrophic scars, hypertrophic scars, and hypopigmented scars.[16] With minimal downtime, non-ablative fractional lasers produce gradual results after a number of treatments, with the most significant improvement noted between 3 and 6 months following the final laser treatment.[2] A study by Tierney et al. comparing 1550-nm Non-ablative fractional laser to 595-nm Pulsed Dye Laser for the treatment of surgical scars showed that Non-ablative fractional laser outperformed Pulse Dye Laser and 83% of patients preferred the half of the scar treated with a non-ablative fractional laser. Niwa et al. examined non-ablative fractional laser in the treatment of hypertrophic scars and found 26% to 75% clinical improvement after two to three treatment sessions done at 4-week intervals.[20] For vascular scars, the Pulsed Dye Laser is particularly useful, and has been shown to improve the appearance by reducing the redness associated with certain types of scarring.
Intense Pulsed Light for Scars
Alongside lasers, high-intensity, non-coherent light sources have been shown to be useful for the treatment of scars. A study by Kontoes et al found that intense pulsed light (IPL) sources, emitting noncoherent, broadband, pulsed light can treat a range of scarring. IPL sources are commonly used in the treatment of vascular and pigmented lesions by targeting haemoglobin and melanin chromophores in accordance with the Theory of Selective Photothermolysis. They can therefore act on the vasculature and the pigmentation of a scar to improve its appearance and/or symptoms that may coexist. It was found that over a 3-year period, patient satisfaction was high following IPL treatment in the majority of cases, and yielded the best results when used in combination with other treatments. This study demonstrated that intense pulsed light treatments are applicable to, and effective in, the treatment of almost all types of scars and can easily be combined with other treatment methods such as Microneedling, and silicone dressings.
Scar Prevention
Using lasers to prevent the formation of scars is a relatively new concept that is gaining popularity in the aesthetic field. Wound edges can be vaporized with either a CO2 or an Er:YAG laser before primary surgical closure to enhance ultimate cosmesis.[9] Alternatively, a 585-nm PDL system can be used to treat surgical sites, traumatic wounds, or ulcerations to reduce the risk of scarring and prevent excessive scar formation.[24 25 26 (Figure 7)].
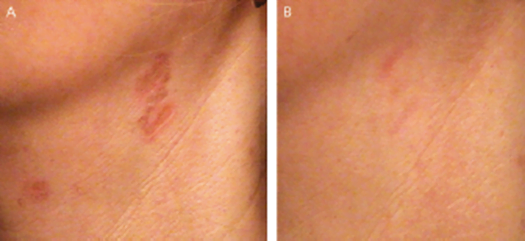
Figure 7. Prescars on the neck before (A) and after PDL treatment (B).
Additional Modalities for Scar Treatments
There are multiple modalities that aim to reduce and improve the appearance of scars that do not use lasers or light including Microneedling, topicals, injectables and more. A brief review of these treatments is listed below.
Microneedling
Microneedling treatment utilises needles to create tiny punctures in the skin in order to initiate the wound healing response. The needles break collagen bundles in the superficial layer of the dermis that are responsible for scars, with subsequent induction of better-structured collagen to reduce the appearance of the scar. Patients often see an improvement in skin appearance and texture. This treatment can be utilised for most kinds of scarring.
Surgery
Scar revision surgery, where existing scar tissue is surgically removed, can be an effective modality that can improve the appearance of scars, transform the shape of the scar and increasing functionality, for example, by releasing a tight scar that is close to a joint in order to improve movement and decrease patient discomfort. Surgical excision of hypertrophic or keloid scars is often used in conjunction with other treatment modalities such as silicone gel sheeting. The key problem with performing surgery on a scar already formed is there is also an increased risk of further keloid and hypertrophic scarring following surgery. After surgery, the recurrence rate for keloid scarring is approximately 50-80%.[27]
Scarring is inevitably unpredictable and excision has an associated downtime and a requirement for local anaesthetic.
Chemical Peels
Chemical Peels are most commonly used for the treatment of acne scars, although they can be utilised for any type of scar which has an element of hypertrophy, to enable the smoothing of the scar to the skin’s surface. Examples would include raised scars created after burns, surgery or trauma. TCA/Phenol strength peels are better suited for deeper scarring however, a lengthy downtime is experienced by patients with stronger peels. Dot peeling with these acids can be used to directly target ice pick or small box scars. Salicylic acid peels are currently the most frequently used and tend to be combined with other treatments such as Microneedling, IPL and laser for the best results. Currently, there appears to be no consensus on the best combination of treatments. However, a series of chemical peels can lead to a significant improvement over a short period, leading to patient satisfaction and maintenance of clinical results.
Plasma Rich Platelet Therapy
Autologous platelet-rich plasma contains a higher concentration of platelets than normally found, in order to enhance wound healing[29 30]. Derived by spinning the patient’s blood and injecting it back into the area of scarring, practitioners are able to deliver a high concentration of growth factors, platelets and cytokines to the target tissue. In response to platelet activation, the alpha-granules of the platelets release growth factors and induce cell proliferation and cell differentiation for tissue regeneration. These growth factors play an important role in controlling and proliferating mesenchymal stem cells, including fibroblasts, and have been shown to induce collagen and matrix component synthesis, which is expected to boost atrophic scars[31.
Additionally, the application of platelet-rich plasma to surgical wounds post-surgery has been shown as an effective pre-scar solution, for the acceleration of tissue repair and for the reduction of postoperative pain[32]. This treatment can be utilised alongside other scar treatment methods mentioned.
Dermabrasion and Microdermabrasion
Dermabrasion/Microdermabrasion was the first major advance treatment of acne scarring. Dermabrasion and microdermabrasion are both facial resurfacing techniques that mechanically remove damaged skin in order to promote remodelling of the skin’s structural proteins. Dermabrasion is ablative, induces more downtime and requires anaesthesia. Dermabrasion eliminates the epidermis entirely and penetrates to the level of the papillary or reticular dermis, causing structural protein remodelling of the skin. A more superficial variation of dermabrasion, microdermabrasion, only removes the outer layer of the epidermis, which accelerates the natural exfoliation process. Dermabrasion techniques can be effective in the treatment of scars and produce clinically significant improvements in skin appearance. Practitioners are, however, unable to treat deep wounds with microdermabrasion procedures[36]. In addition, dermabrasion does not optimally enhance ice selection or deep boxcar scars and although microdermabrasion may help those with uneven skin texture or congested skin, it has limited efficacy in the treatment of scars.
Platelet-rich Plasma
Autologous platelet-rich plasma contains a higher concentration of platelets than normally found, so as to enhance wound healing (Fennis et al, 2002; Carter et al, 2003). Derived by spinning the patient’s blood and injecting it back into the area of scarring, practitioners are able to deliver a high concentration of growth factors, platelets and cytokines to the target tissue. In response to platelet activation, the alpha granules of the platelets release growth factors and induce cell proliferation and cell differentiation for tissue regeneration. These growth factors play an important role in controlling and proliferating mesenchymal stem cells, including fibroblasts, and have been shown to induce collagen and matrix component synthesis, which is expected to boost atrophic scars (Ibrahim et al, 2017). Additionally, the application of platelet-rich plasma to surgical wounds post-surgery has been shown as an effective pre-scar solution, for the acceleration of tissue repair and for the reduction of postoperative pain (Gardner et al, 2007). This treatment can be used alongside other scar treatment methods that are mentioned in this article.
Steroid Injections
Steroid injections are often the first line of defence in the prevention and treatment of keloids and hypertrophic scars from a medical perspective. Usually, triamcinolone is injected along the length of the wound. The result is a reduction in the redness of the scar and then slowing of growth, followed in most cases by regression of the bulk of the lesion. Corticosteroid injections can have improved efficacy when combined with other therapies, including lasers. Furthermore, triamcinolone injections have also been shown to improve scars via inhibition of fibroblast proliferation, decreased collagen synthesis, and inhibition of collagenase inhibitors. While triamcinolone’s side effects, including skin atrophy, telangiectasia, and hypopigmentation, are well known, lower doses of steroids can decrease these effects.
Psychological Considerations When Treating Scars
Finally, aesthetic practitioners should consider the psychological implications of patients when treating scars. Patients with facial scars such as acne scarring appear to experience low self-esteem, to be nervous about their condition, and to be unrealistic about the results of care. As practitioners, it is crucial to have a mindful discussion with a thorough description of the treatment, its consequences and potential results when treating any form of scars.
Through doing this you can gain the patient’s confidence and strengthen the relationship between the medic and the patient. For the effectiveness of the process, this relationship is important. Therefore, when reviewing expectations/concerns and past experiences with treating scars using a variety of modalities, all aesthetic practitioners must be cautious and must be pragmatic about outcomes and complications to maximise patient satisfaction.
Conclusion
With the range of modalities available for the treatment of scars, practitioners have the ability to create a treatment plan tailored to the patient needs, that may utilise a combination of treatments. Traditional treatments such as silicone dressings and intralesional steroid injections still have an important role to play, but optimal results can be obtained when combing these methods with other modalities such as laser and light sources.
Before and After Scar Treatment






Contact The Lynton Clinic Today
If you would like to find out more about how we can treat your Scarring, click to book a consultation.